{kind=link}

LISTEN TO STORY
WATCH STORY
By: Isuru Parakrama
March 30, Colombo (LNW): A newly identified COVID-19 subvariant, known scientifically as BA.3.2 and informally dubbed “Cicada”, is drawing increasing global attention as health authorities monitor its spread and unusual genetic profile.
First detected in South Africa in November 2024, the variant has now been identified in more than 23 countries across five continents, underscoring the continued evolution of the SARS-CoV-2 virus.
Despite the growing scrutiny, experts caution against alarm. Current evidence suggests that while Cicada is highly mutated and potentially more capable of evading immunity, it does not appear to cause more severe illness than earlier variants such as Delta or Omicron.
At the centre of scientific concern is Cicada’s mutation profile. The variant carries between 70 and 75 mutations in its spike protein alone—significantly higher than the 30 to 40 mutations typically seen in recent strains. This spike protein is critical, as it enables the virus to bind to human cells and is the primary target of existing vaccines.
The scale of these mutations has led researchers to describe the variant as “highly genetically divergent”, raising questions about how effectively current immunity—whether from vaccination or prior infection—can respond.
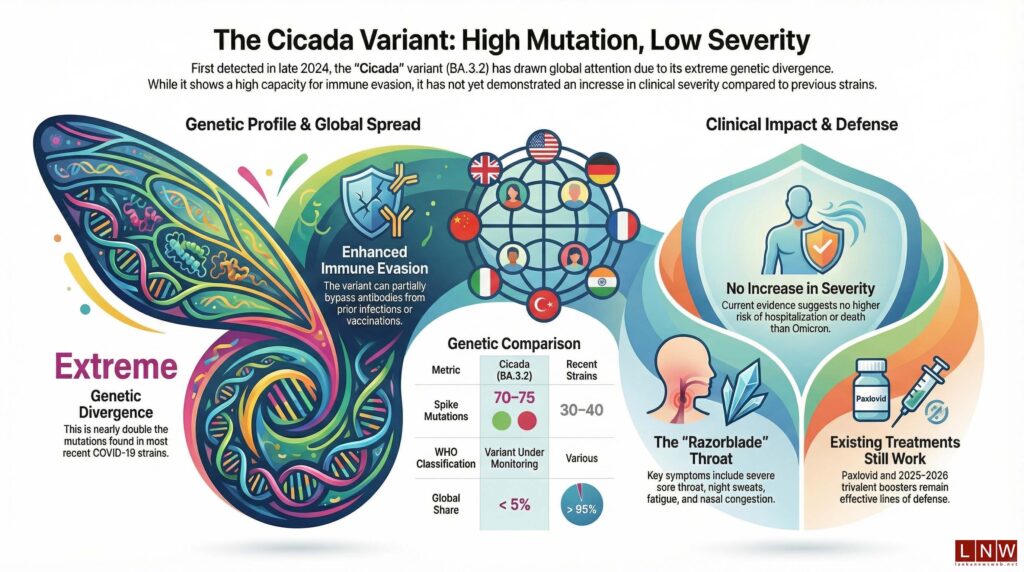
Laboratory studies have already indicated that Cicada demonstrates enhanced immune escape. In practical terms, this means the variant can partially bypass antibodies generated by existing COVID-19 vaccines or past infections, increasing the likelihood of reinfection. However, scientists emphasise that immune escape does not automatically translate into more severe disease.
Clinically, Cicada appears to mirror the symptoms associated with Omicron and its subvariants. Patients typically report a runny or blocked nose, sneezing, a severe sore throat—often described as a “razorblade throat”—alongside cough, fatigue, headaches, muscle aches, and night sweats. While these symptoms can be uncomfortable, there is no evidence thus far to suggest an increase in hospitalisations or mortality linked specifically to this variant.
The World Health Organisation (WHO) has classified BA.3.2 as a “Variant Under Monitoring” (VUM), the lowest level in its tracking system. This designation indicates that while the variant’s mutations warrant observation, there is currently no confirmed evidence of increased public health risk. Health authorities, including the CDC, stress that surveillance efforts are focused primarily on understanding its immune evasion capabilities rather than responding to any heightened severity.
Geographically, Cicada’s spread has been notable but uneven. It has gained particular traction in parts of Europe, where it accounted for roughly 30 per cent of sequenced cases in countries such as Denmark, Germany, and the Netherlands between late 2025 and early 2026.
Nevertheless, its global share remains relatively low—estimated at under 5 per cent of sequenced cases—though experts caution that limited genomic surveillance in many regions may mask its true prevalence.
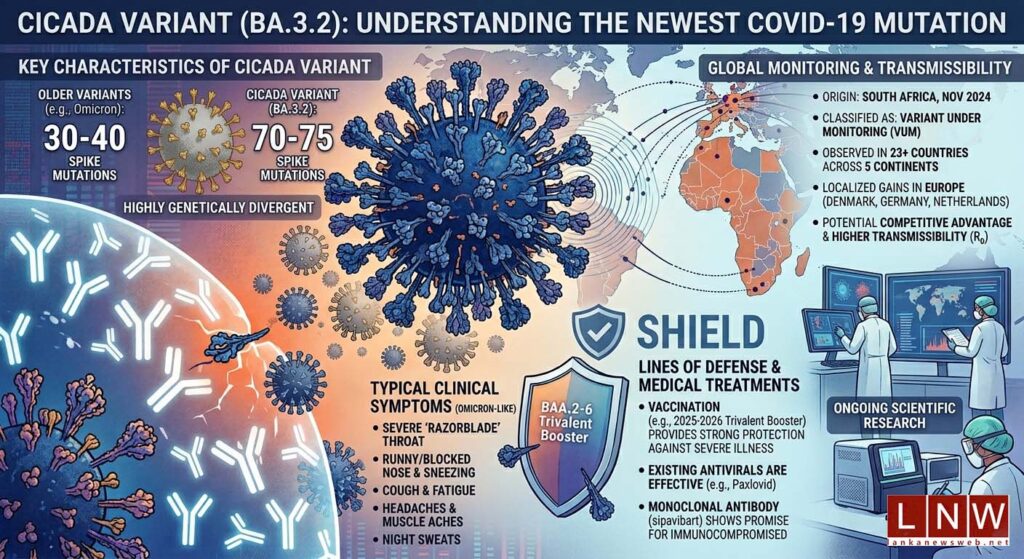
Another area of active research is transmissibility. While no definitive reproduction number (R₀) has yet been published, early indicators suggest the variant may have a competitive advantage, particularly due to its immune escape properties. This could allow it to spread more easily in populations with existing immunity, even if it is not inherently more infectious in the traditional sense.
Vaccination remains a key line of defence, albeit with some caveats. Laboratory findings show reduced antibody neutralisation against Cicada compared to other circulating strains. However, vaccines—particularly the 2025–2026 trivalent booster—are still expected to provide meaningful protection, especially against severe illness. Real-world effectiveness data is still being gathered, leaving some uncertainty about the full extent of vaccine performance against this variant.
Encouragingly, existing antiviral treatments continue to hold up. Paxlovid remains effective, and the monoclonal antibody therapy sipavibart has shown preserved activity against the variant, offering a crucial option for immunocompromised individuals who may not respond well to vaccines.
For the general public, health guidance remains largely unchanged. Authorities recommend staying up to date with booster vaccinations, remaining vigilant for symptoms, and testing when necessary. High-risk groups—including the elderly and those with underlying health conditions—are advised to take additional precautions and consult healthcare providers for tailored protection strategies.
What remains unknown, however, is just as important. Scientists are still investigating the variant’s true transmissibility, the duration of immunity following infection, and its long-term clinical impact. These gaps highlight the ongoing need for robust genomic surveillance and international data sharing.
In essence, the Cicada variant represents a familiar yet evolving challenge. It underscores the virus’s capacity to adapt, but also the resilience of global public health systems that have learned to respond with vigilance rather than panic. For now, the message from experts is clear: stay informed, stay protected, and recognise that while the virus continues to change, the tools to manage it remain firmly in place.
*All information compiled from CDC, WHO, peer-reviewed publications, and reputable news sources dated March 2026.
